Overview
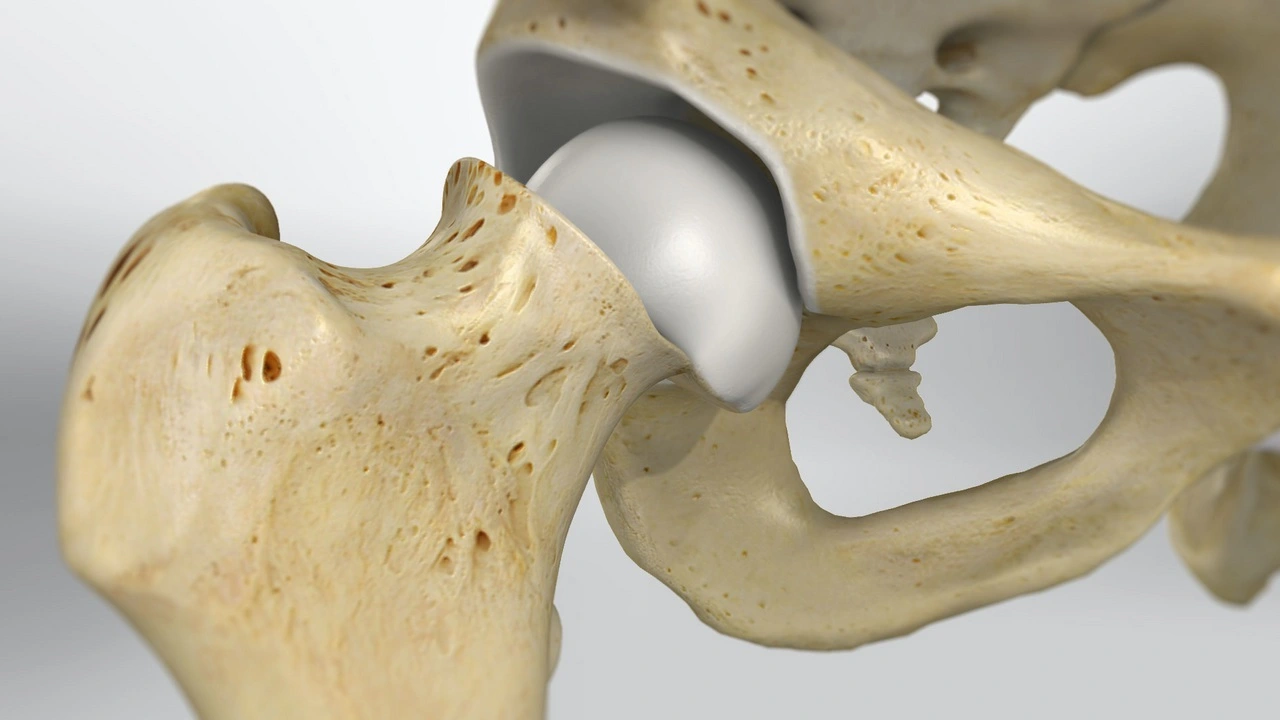
Slipped Capital Femoral Epiphysis (SCFE) is one of the most frequently encountered hip disorders in children and adolescents, particularly during the rapid phases of growth that occur around puberty. In this condition, the head of the femur (the ball-shaped top portion of the thigh bone) gradually shifts away from its normal alignment with the femoral neck at the growth plate (also called the physis).
Since the growth plate is a relatively weaker zone compared to the surrounding bone structures, it becomes the most vulnerable site for such slippage.
To visualize the problem, many experts describe it as an “ice cream slipping off its cone,” where the ball of the hip joint (femoral head) stays seated inside the socket of the pelvis, but its alignment with the femoral neck becomes disrupted due to gradual displacement. This shift is not just painful but also mechanically destabilizing, affecting how the hip supports body weight and movement.
Slipped Capital Femoral Epiphysis is classified as an orthopedic emergency because untreated slippage can result in serious complications. Progressive displacement of the femoral head can damage the blood supply to the bone, leading to avascular necrosis, chronic hip deformity, early-onset osteoarthritis, and even lifelong disability. Because the symptoms can sometimes mimic knee pain or general leg discomfort, many cases are misdiagnosed or detected late, which increases the risk of long-term issues.
Early recognition and timely treatment are absolutely crucial for preserving hip function and preventing permanent complications. That’s why clinics such as DMPhysios in Noida, which specialize in managing spine and sports-related conditions with a strong emphasis on patient-centered rehabilitation, are vital in the treatment pathway. Our comprehensive approach combines medical collaboration, physiotherapy, and personalized care strategies to help children and adolescents recover safely, regain mobility, and return to daily activities without fear of chronic disability.
Symptoms
The symptoms of Slipped Capital Femoral Epiphysis can vary depending on the severity and chronicity of the condition. Common symptoms include:
- Hip pain: Often described as dull or aching, localized to the groin, thigh, or even the knee.
- Limping: One of the earliest signs; children may present with an antalgic gait to reduce hip discomfort.
- Restricted range of motion: Particularly internal rotation, abduction, and flexion of the hip.
- Referred knee pain: Many children initially present with knee pain, which may delay diagnosis.
- Shortening or external rotation of the affected leg: In severe cases, the leg may appear shorter and turned outward.
- Difficulty walking or inability to bear weight: Seen in unstable Slipped Capital Femoral Epiphysis, requiring urgent medical intervention.
Early recognition of these symptoms is essential, and physiotherapists at DMPhysios are trained to detect biomechanical changes during movement assessments that may suggest Slipped Capital Femoral Epiphysis.
Types of Slipped Capital Femoral Epiphysis
Slipped Capital Femoral Epiphysis can be classified in several ways depending on stability, chronicity, or severity:
- Based on Stability:
- Stable Slipped Capital Femoral Epiphysis: The patient can still bear weight on the affected leg, with or without crutches.
- Unstable Slipped Capital Femoral Epiphysis: The patient cannot bear weight at all. This is a surgical emergency with a higher risk of complications such as avascular necrosis.
- Based on Duration (Chronicity):
- Acute Slipped Capital Femoral Epiphysis: Symptoms occur suddenly, typically less than 3 weeks.
- Chronic Slipped Capital Femoral Epiphysis: Symptoms develop gradually over weeks or months; the most common type.
- Acute-on-Chronic Slipped Capital Femoral Epiphysis: A child has long-standing symptoms but then develops a sudden worsening due to a fresh slip.
- Based on Severity (Degree of Slip):
- Mild: Less than 30° of slippage.
- Moderate: Between 30° and 50°.
- Severe: Greater than 50°.
This classification helps guide treatment and prognosis.
Causes
The exact cause of Slipped Capital Femoral Epiphysis is multifactorial, but the main factor is mechanical stress on a weakened growth plate during puberty. Some common contributing factors include:
- Rapid growth spurts during adolescence, when the physis is most vulnerable.
- Endocrine abnormalities such as hypothyroidism, growth hormone abnormalities, or diabetes.
- Mechanical loading: Overweight or obese children have higher mechanical stress across the hip joint.
- Trauma: Though rare, a fall or injury can precipitate a slip.
- Genetic predisposition: Family history can increase risk.
Risk Factors
Certain children are at higher risk of developing Slipped Capital Femoral Epiphysis. Key risk factors include:
- Age: Most commonly seen between ages 10–16 years.
- Gender: Boys are more frequently affected than girls.
- Obesity: A major risk factor due to increased load on the hip.
- Endocrine conditions: Hypothyroidism, hypogonadism, and pituitary disorders increase susceptibility.
- Bilateral involvement: Up to 40% of cases may affect both hips, either simultaneously or sequentially.
- Family history: A genetic predisposition may be involved in some children.
Treatment
The cornerstone of Slipped Capital Femoral Epiphysis treatment is surgical stabilization to prevent further slippage and protect the hip joint. Common treatment methods include:
- In-situ fixation: A single screw is inserted to stabilize the femoral head and prevent further displacement. This is the most common surgical method for stable Slipped Capital Femoral Epiphysis.
- Open reduction and internal fixation: Required in severe or unstable Slipped Capital Femoral Epiphysis where the femoral head has displaced significantly.
- Prophylactic pinning of the opposite hip: Sometimes recommended due to the high risk of bilateral involvement.
After surgery, rehabilitation becomes critical. This is where clinics like DMPhysios in Noida excel by providing structured, patient-centered physiotherapy care to ensure safe recovery and restore normal function.
Physiotherapy Treatment
Physiotherapy is vital in the recovery phase following surgical management of Slipped Capital Femoral Epiphysis. At DMPhysios, treatment is individualized, focusing on restoring mobility, improving strength, and enhancing long-term hip function.
1. Early Postoperative Phase (Weeks 1–4):
- Pain management: Cryotherapy and gentle positioning to reduce inflammation.
- Protected weight bearing: Crutches or walker until advised otherwise by the surgeon.
- Gentle range-of-motion exercises: Only within safe limits, avoiding excessive rotation.
- Quadriceps and gluteal isometrics: To maintain muscle activation and prevent atrophy.
2. Intermediate Phase (Weeks 4–8):
- Gradual progression to partial and then full weight-bearing as tolerated.
- Hip strengthening: Focus on hip abductors, extensors, and core muscles with resistance bands and closed-chain exercises.
- Gait training: Correcting limping patterns with functional re-education.
- Aquatic therapy: Low-impact strengthening and mobility restoration.
3. Advanced Rehabilitation Phase (Weeks 8–16):
- Dynamic strengthening: Incorporating squats, step-ups, and bridging exercises.
- Balance and proprioceptive training: Using stability boards or single-leg stance exercises.
- Functional retraining: Gradual return to sports-specific or daily activities.
- Flexibility work: Gentle stretching of hip flexors, hamstrings, and quadriceps.
4. Long-Term Management:
- Education on joint protection strategies.
- Lifestyle modifications, especially weight management, to reduce stress on the hip.
- Monitoring for complications such as avascular necrosis or early osteoarthritis.
At DMPhysios, therapists ensure patient progress is closely monitored with reassessment at every stage. Their patient-centered rehabilitation model emphasizes active involvement of children and parents in the recovery journey.
Prevention
While Slipped Capital Femoral Epiphysis cannot always be prevented, certain strategies may reduce risk or allow early detection:
- Weight management: Maintaining a healthy weight reduces excessive stress on the hip.
- Regular screening: Children with endocrine conditions or a family history should be monitored closely.
- Early medical evaluation: Any child with unexplained hip, thigh, or knee pain should be evaluated for Slipped Capital Femoral Epiphysis.
- Avoiding high-impact activities during growth spurts if hip pain is present.
Preventive care and early diagnosis play an important role in reducing long-term complications.
Conclusion
Slipped Capital Femoral Epiphysis is a serious adolescent hip condition that requires urgent attention and a structured treatment plan. With early diagnosis, surgical stabilization, and comprehensive rehabilitation, most children can return to normal, active lives.
At DMPhysios in Noida, a leading clinic for spine and sports conditions, the focus is always on patient-centered rehabilitation. Their expert physiotherapists provide tailored exercise programs, progressive recovery plans, and long-term guidance to ensure children regain confidence, mobility, and function after Slipped Capital Femoral Epiphysis.If your child is experiencing hip or knee pain, limping, or restricted hip movement, do not ignore the signs. Early consultation with specialists at DMPhysios can make a life-changing difference in preventing long-term disability.