Overview
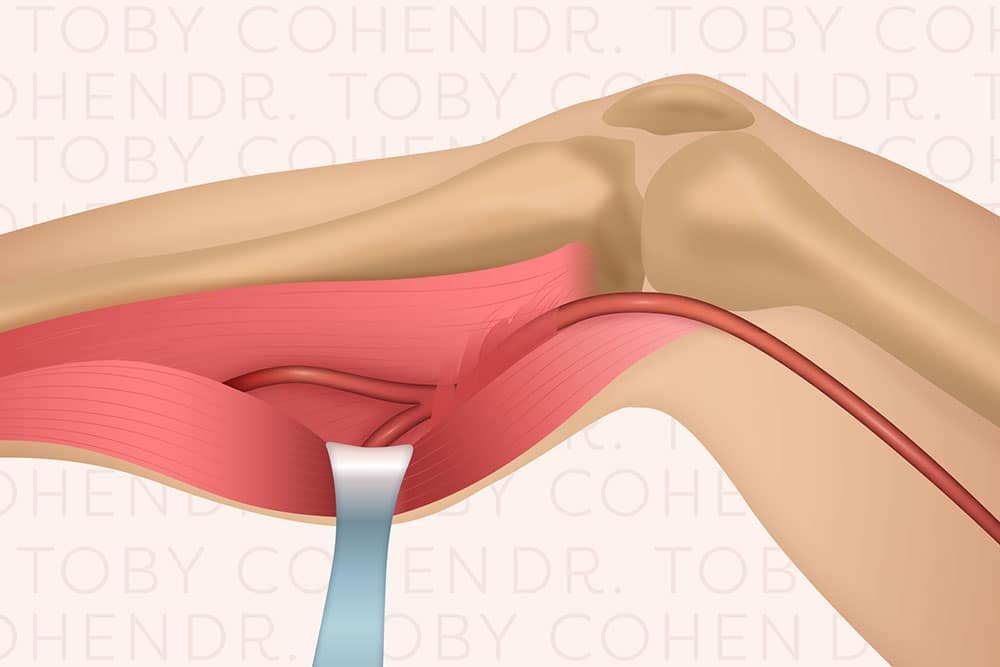
Popliteal Artery Entrapment Syndrome (PAES) is a rare but significant vascular condition that affects the circulation in the lower leg. It occurs when the popliteal artery—the major blood vessel behind the knee—becomes compressed or entrapped by surrounding muscles, tendons, or other soft tissue structures. This entrapment restricts blood flow to the lower leg, especially during physical activity, leading to symptoms such as pain, cramping, or even numbness in the calf and foot.
Unlike atherosclerosis or blood clot-related vascular issues, Popliteal Artery Entrapment Syndrome often develops in young, healthy, and athletic individuals who otherwise have no risk factors for vascular disease. Because of its unique mechanism, it is frequently misdiagnosed as a musculoskeletal condition, which makes early recognition and proper management crucial.
At DMPhysios, a leading clinic in Noida for spine and sports conditions with patient-centered rehabilitation, accurate assessment and individualized treatment strategies are emphasized to ensure patients with Popliteal Artery Entrapment Syndrome receive the right care.
Symptoms
The clinical presentation of Popliteal Artery Entrapment Syndrome can vary but typically includes symptoms triggered by activity and relieved by rest. Common symptoms are:
- Exertional calf pain: Often described as cramping or aching during exercise, especially running or climbing stairs.
- Numbness or tingling: Reduced blood supply can cause sensory disturbances in the foot.
- Coldness in the foot or toes: Due to impaired circulation.
- Weakness in the calf: In severe cases, reduced blood flow affects muscle performance.
- Swelling or tightness sensation: Particularly after prolonged activity.
- Diminished or absent pulses in the foot: Notable when the ankle is positioned in plantarflexion (foot pointed downward).
Because these symptoms often mimic shin splints, compartment syndrome, or nerve entrapment, Popliteal Artery Entrapment Syndrome may be overlooked without proper vascular assessment.
Types of Popliteal Artery Entrapment Syndrome
Popliteal Artery Entrapment Syndrome is classified into several anatomical types depending on the structural anomaly causing compression:
- Type I – The popliteal artery follows an abnormal course around the medial head of the gastrocnemius muscle.
- Type II – The medial head of the gastrocnemius muscle is abnormally positioned, displacing the artery.
- Type III – An accessory slip of the gastrocnemius compresses the artery.
- Type IV – The artery is compressed by the popliteus muscle or fibrous bands.
- Type V – Both the popliteal artery and vein are entrapped.
- Functional PAES – No anatomical abnormality is present, but muscle hypertrophy (usually in athletes) leads to dynamic compression of the artery during activity.
This classification is important as it guides both diagnosis and treatment planning.
Causes
The causes of PAES can be structural or functional:
- Congenital anomalies: Abnormal development of muscles and tendons in the calf region can predispose individuals to arterial compression.
- Muscular hypertrophy: Athletes with well-developed calf muscles are more prone to functional entrapment.
- Repetitive movements: Activities involving frequent running, jumping, or cycling increase mechanical pressure on the popliteal artery.
- Fibrous tissue bands: These can tether and restrict the artery.
Risk Factors
Certain populations are more vulnerable to developing Popliteal Artery Entrapment Syndrome. These include:
- Young athletes: Especially runners, footballers, and cyclists who perform high-demand leg activities.
- Males: The condition is more common in men, often due to higher rates of muscular hypertrophy.
- Individuals with anatomical variations: Congenital differences in calf muscle or tendon structures predispose to entrapment.
- People with repetitive lower limb stress: Occupational or sports-related stress that involves frequent knee extension and flexion.
Treatment
Treatment depends on the severity and underlying anatomical cause:
- Conservative Management
- Reserved for mild or functional cases.
- Includes activity modification, physiotherapy, and careful monitoring.
- Surgical Management
- Indicated in anatomical entrapments or severe symptoms.
- Procedures include muscle or tendon release to decompress the artery, or in advanced cases, vascular reconstruction to repair damage to the artery.
- Post-surgical Rehabilitation
- Essential for restoring mobility, strength, and circulation.
- Tailored physiotherapy programs help prevent recurrence and improve athletic performance.
Physiotherapy Treatment
Physiotherapy plays a vital role both before and after surgical intervention. At DMPhysios, physiotherapists design structured and progressive rehabilitation plans with a patient-centered approach. The main physiotherapy interventions include:
1. Education and Activity Modification
- Patients are educated about avoiding aggravating activities such as sprinting or deep squatting in the early stages.
- Gradual return-to-sport strategies are discussed.
2. Flexibility Training
- Stretching exercises for the gastrocnemius, soleus, and hamstring muscles to reduce undue tension on the artery.
- Dynamic mobility drills to improve knee and ankle range of motion.
3. Strengthening Programs
- Focus on balanced strengthening of lower limb muscles to prevent dominance of hypertrophied gastrocnemius.
- Closed-chain exercises like squats, lunges, and step-ups (initially modified).
- Gradual progression to sport-specific strengthening.
4. Neurovascular Gliding and Circulatory Exercises
- Gentle nerve and artery mobilization techniques to enhance blood flow and reduce compression.
- Calf pump exercises and ankle circles to improve venous return and arterial circulation.
5. Gait and Biomechanical Correction
- Assessment of running or walking patterns to reduce strain on the popliteal artery.
- Use of orthotics if abnormal foot mechanics are contributing.
6. Post-Surgical Rehabilitation
- Early mobilization and pain control with modalities such as cryotherapy or TENS.
- Gradual strengthening and functional retraining, ensuring no recurrence of symptoms.
- Return-to-sport testing to ensure safe participation in athletic activities.
By combining clinical expertise with individualized rehabilitation strategies, DMPhysios in Noida provides effective physiotherapy care for patients recovering from Popliteal Artery Entrapment Syndrome.
Prevention
While not all cases can be prevented—especially congenital ones—certain steps may reduce risk:
- Gradual training progression: Avoid sudden increases in intensity or mileage during running or sports.
- Balanced strengthening: Work on both agonist and antagonist muscles to prevent hypertrophy-related imbalances.
- Proper warm-up and cool-down: Dynamic stretching before activity and static stretching afterward.
- Monitoring symptoms: Seek evaluation if calf pain persists despite rest.
- Biomechanical assessment: Correct gait abnormalities early with the help of physiotherapists.
Conclusion
Popliteal Artery Entrapment Syndrome is a challenging vascular condition that often affects young, athletic individuals. Early recognition and accurate diagnosis are crucial since symptoms can mimic other musculoskeletal or nerve-related conditions. With proper treatment—whether conservative management, surgery, or physiotherapy—patients can return to an active and pain-free lifestyle.
At DMPhysios, a Noida-based clinic specializing in spine and sports conditions, patient-centered rehabilitation ensures that every case of Popliteal Artery Entrapment Syndrome receives comprehensive care. Through expert physiotherapy intervention, education, and progressive rehabilitation, patients not only recover but also prevent recurrence, regaining confidence in their athletic performance.If you or someone you know is struggling with calf pain, numbness, or circulation issues that worsen during exercise, don’t ignore the signs. Reach out to DMPhysios for specialized care and start your journey towards recovery with a team that puts patient well-being first.