Why Your Knees Hurt Even When There’s “Nothing on the X-Ray”
Article Overview
- Quick Headline Takeaways
- Why An X-ray Can Be “Normal” While Your Knee Hurts
- How Clinicians Figure Out What’s Really Happening
- Evidence-based Treatments That Actually Work
- Special Focus: Patellofemoral Pain Syndrome (PFPS)
- When To Worry: Red Flags Requiring Urgent Attention
- A Practical Roadmap You Can Start Today
- Common Patient Questions
- How DMPhysios Approaches “Normal X-ray, Painful Knee”
- Final words


Y
ou’ve been told: “Your X-ray looks fine, there’s nothing structural to explain your pain.” And yet your knee aches climbing stairs, throbs after a run, or catches when you squat.
That contradiction is confusing and frustrating, but it’s also common. X-rays are a powerful tool, but they’re limited. This deep-dive explains, with research-backed clarity and practical steps you can use today, why pain and X-ray findings sometimes don’t match, and what actually helps. If you’re in Noida or nearby, DMPhysios can help you walk through this clinically and compassionately; their approach focuses on functional recovery and evidence-based rehabilitation.
Quick Headline Takeaways
- An X-ray shows bone and joint space but misses many soft-tissue and early cartilage problems.
- Common pain generators not seen on X-ray include patellofemoral overload, tendinopathy, bursitis, muscle or biomechanical dysfunction, and early cartilage or meniscal degeneration visible on MRI.
- Pain is not always proportional to tissue damage. Central sensitization and nociplastic pain can make a knee feel painful despite minimal imaging changes.
- High-quality evidence supports exercise and targeted physiotherapy as first-line treatments for most chronic knee pain presentations, even when X-rays look normal.
Why An X-ray Can Be “Normal” While Your Knee Hurts
Here’s what an X-ray actually shows: bone outlines, the distance between bones (joint space as an indirect sign of cartilage loss), large bone spurs (osteophytes), and gross alignment. It does not show soft tissues (tendons, ligaments, cartilage biochemistry), small meniscal tears, bone marrow lesions, or subtle cartilage wear. MRI and ultrasound are far more sensitive for those structures. That mismatch between what we image and what’s hurting is the first reason for the “normal X-ray, painful knee” scenario.
Common Causes That X-rays Miss
- Patellofemoral Pain Syndrome (PFPS) or Anterior Knee Pain
PFPS is driven by overload of the patella on the femur and by muscle imbalance or biomechanics rather than bone abnormalities. X-rays can be normal. Diagnosis is clinical. - Tendinopathies of the patellar tendon, quadriceps tendon or pes anserinus
Tendon irritation or overload usually shows on ultrasound or MRI but not on plain radiographs. - Iliotibial Band (ITB) Friction Syndrome And Bursitis
Involves soft-tissue irritation and inflammation and cannot be identified on X-ray. - Early Meniscal Degeneration Or Small Tears
Many of these do not change the appearance of the X-ray but can be pain generators. MRI is more sensitive but its findings must be clinically correlated. - Referred Pain from the hip or lumbar spine
Hip pathology or nerve root irritation may produce knee pain even when the knee is structurally normal on X-ray.
Nociplastic Or Centrally Facilitated Pain
This occurs when the nervous system amplifies pain signals. Even small tissue insults can feel severe because of altered central processing.
Important Nuance: Imaging Findings Do Not Always Equal Symptoms
Large studies show that MRI features often occur in people with no knee pain. Many asymptomatic adults have meniscal tears or cartilage lesions on MRI. Conversely, people with significant pain may show only minimal radiographic change. This is why treatment decisions must be based on a careful history and physical exam, not on imaging alone.
How Clinicians Figure Out What’s Really Happening
If your X-ray is normal but you still hurt, clinicians use a structured process.
1. Detailed History
Pain location (front, inner, outer, behind kneecap), triggers (stairs, squatting, running), pain character (aching, sharp, catching), trauma history, loading patterns, sleep and psychosocial factors all contribute essential diagnostic clues.
2. Physical Examination
Movement analysis (squat, step down, single-leg tasks), strength testing of quadriceps and hip musculature, palpation of tendons or bursae, special tests for meniscus and ligaments, and assessment of hip and lumbar spine are key.
DMPhysios emphasizes this functional assessment and tailors care to findings rather than scans.
3. Selective Imaging
If soft-tissue pathology is suspected or conservative care fails, MRI or ultrasound may be ordered. These modalities detect meniscal pathology, tendon tears, cartilage lesions or inflammatory changes that X-rays cannot reveal.
4. Pain Phenotype Identification
Clinicians determine whether symptoms are nociceptive (tissue irritation), neuropathic (nerve-related), or nociplastic (central sensitization). Identifying the right pain mechanism improves treatment accuracy.
Evidence-based Treatments That Actually Work
1. Exercise Therapy And Strength Training
Strong evidence from systematic reviews shows that exercise reduces knee pain and improves function for a wide variety of knee conditions.
Programs target quadriceps strength, hip abductors, neuromuscular control and progressive loading. DMPhysios builds structured, individualized programs with weekly progressions.
2. Load Management And Activity Modification
Pain often results from repeated overload. Short-term reduction in aggravating activities (like deep squats or downhill running) helps calm symptoms while maintaining overall movement. Gradual re-loading is essential for tendinopathy and PFPS recovery. DMPhysios teaches optimal loading strategies without deconditioning.
3. Manual Therapy, Soft-tissue Techniques And Education
Joint mobilizations, soft-tissue therapy and myofascial release often reduce short-term pain and improve movement. Education about pain mechanisms reduces fear and improves long-term outcomes, especially when central sensitization is involved.
4. Taping, Bracing And Orthotics
Patellar taping can temporarily reduce pain for PFPS. Foot orthoses help if foot mechanics increase knee loading. These tools support but do not replace exercise therapy.
5. Imaging-guided Injections And Referral Options
If conservative care fails or imaging reveals a specific lesion suitable for injection, corticosteroid or platelet-rich plasma injections may be considered. Surgical referral is reserved for structural issues such as unstable meniscal tears or advanced cartilage damage.
DMPhysios works with orthopedists when multidisciplinary management is needed.
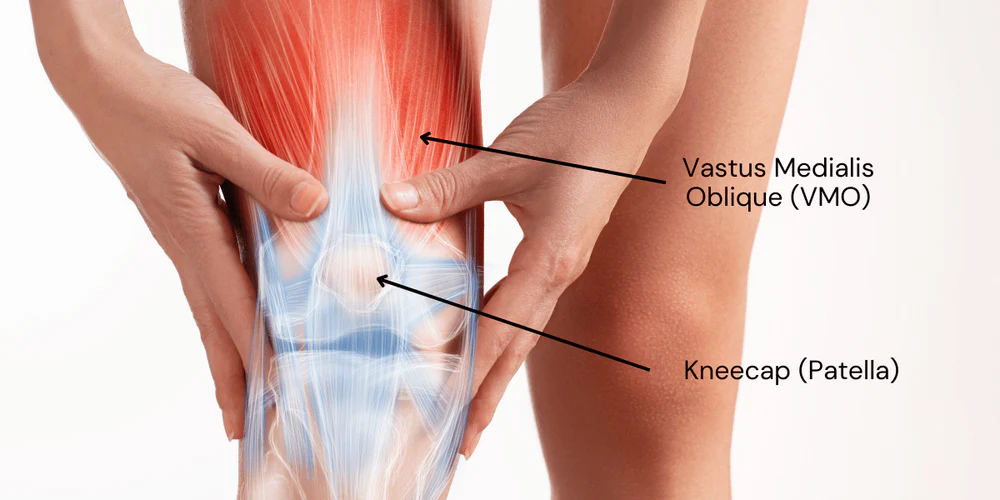
Special Focus: Patellofemoral Pain Syndrome (PFPS)
PFPS is one of the most common reasons for knee pain with a normal X-ray.
Symptoms include:
- Pain during running
- Pain while descending stairs
- Discomfort while sitting for long periods
- Pain during squatting
Best-practice guidelines emphasize strengthening of the quadriceps and hip muscles, movement retraining and controlled progressive loading. DMPhysios follows evidence-based PFPS protocols that include biomechanics correction, taping when needed and structured progressions.
When To Worry: Red Flags Requiring Urgent Attention
Seek immediate medical care if you experience:
- Severe swelling and inability to bear weight after trauma
- Sudden deformity or mechanical locking
- Signs of infection (fever, redness, warmth, severe pain)
- Progressive neurological symptoms such as numbness or weakness
These situations require prompt medical evaluation and possibly advanced imaging.
A Practical Roadmap You Can Start Today
- Track your symptoms
Monitor pain patterns and triggers for 1 to 2 weeks. This helps clinicians understand load tolerance. - Short-term load reduction
Avoid high-aggravation activities temporarily but do not stop moving entirely. - Begin basic strengthening
Isometric quadriceps contractions, straight leg raises and mini-squats often form the starting point of rehabilitation. DMPhysios uses graded progressions based on symptom response. - Schedule a clinical assessment
A physiotherapist can identify movement faults, strength deficits and loading errors that explain your symptoms. DMPhysios provides detailed movement analysis to pinpoint these issues.
Address sleep and stress
Poor sleep and high stress amplify pain. Sleep hygiene, breathing practices and education help calm the nervous system and reduce sensitivity.
Why “No X-ray Findings” Is Not A Dismissal
A normal X-ray does not mean nothing is wrong. It simply means the problem lives in structures that X-rays cannot see or in how the knee is being loaded. Strength deficits, mobility issues, tendon health, movement patterns and nervous system sensitivity all play roles in pain. Physiotherapy targets these factors directly.
DMPhysios specializes in translating scientific evidence into practical rehabilitation steps that restore strength, mobility and confidence.
Common Patient Questions
Q: Do I need an MRI if my X-ray is normal?
Not necessarily. MRI is helpful when soft-tissue injury is suspected or when symptoms persist despite rehabilitation. It should complement a clinical exam, not replace it.
Q: My MRI shows a meniscal tear but my X-ray was normal. Do I need surgery?
Many meniscal tears, especially degenerative ones, improve with physiotherapy alone. Surgery is considered only when there is true mechanical locking or persistent dysfunction.
Q: Is pain in my head when imaging is normal?
No. Pain is always real. Sometimes the nervous system becomes more sensitive, which amplifies pain signals. Education, graded loading and movement retraining help significantly. DMPhysios teaches patients how to understand and manage these mechanisms.
Key Research Insights
- Exercise reduces knee pain and improves function in conditions ranging from osteoarthritis to PFPS.
- MRI detects soft-tissue and cartilage abnormalities that X-rays miss, but findings must match clinical symptoms.
- Central sensitization plays a major role in chronic knee pain and responds well to education and graded activity.
How DMPhysios Approaches “Normal X-ray, Painful Knee”
- Comprehensive functional assessment
- Personalized, progressive exercise program
- Education about pain and load
- Hands-on therapy when appropriate
- Collaboration with orthopedists and radiologists if further imaging or treatment is needed
DMPhysios combines clinical expertise, research-driven protocols and personalized care to help patients return to daily activities and sports with confidence.
Final words
A normal X-ray is not the end of the story. It is simply the beginning of a deeper, more precise assessment. Most people with knee pain and a normal X-ray improve with targeted physiotherapy, which corrects the underlying issues in strength, movement, tendon health and load tolerance.
If you want expert assessment or a tailored rehabilitation plan, DMPhysios offers evidence-based care that focuses on long-term recovery and functional freedom.