Overview
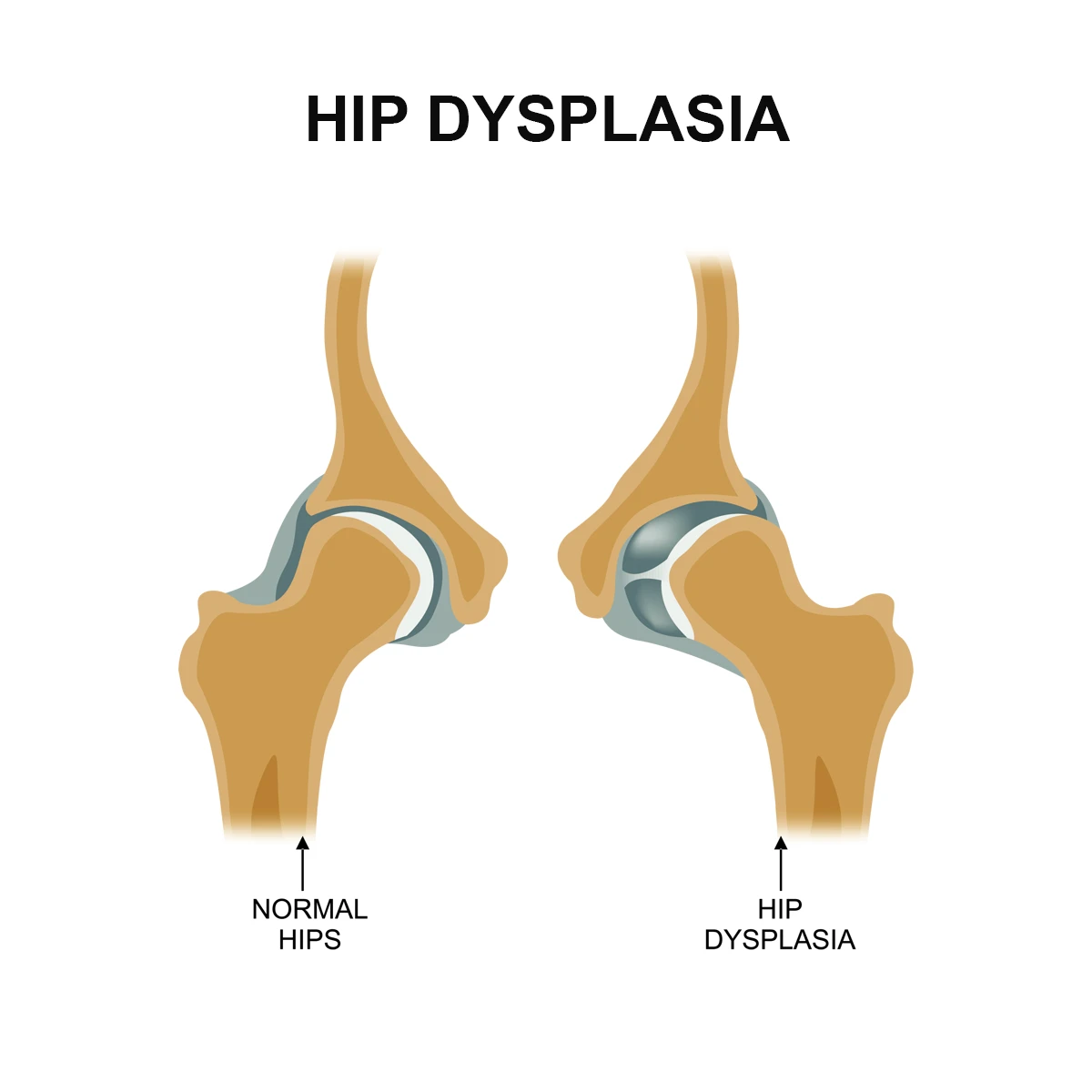
Congenital Dysplasia of Hip (CDH), also known as Developmental Dysplasia of the Hip (DDH), is a musculoskeletal disorder that occurs when the hip joint fails to form properly during fetal development or in the early stages of life. In a normally developed hip, the rounded femoral head (the top of the thigh bone) fits snugly into the acetabulum (the hip socket), allowing smooth, stable, and pain-free movement.
However, in congenital dysplasia of hip, this natural alignment is disrupted—the socket may be too shallow, the joint capsule too loose, or the femoral head may not be positioned correctly within the socket. As a result, the hip joint can become unstable, partially dislocated (subluxated), or even completely dislocated in more severe cases.
The condition can range across a broad spectrum. Some infants may only show mild instability that resolves over time with proper positioning, while others may have a severe and persistent dislocation requiring medical or surgical correction. If congenital dysplasia of hip is not diagnosed and treated at an early stage, it can significantly affect joint health, leading to long-term complications such as altered gait patterns, pain with movement, reduced flexibility, early-onset osteoarthritis, and permanent mobility limitations. This is why early detection through neonatal and infant screening programs is strongly recommended worldwide, as timely intervention has been shown to dramatically improve outcomes.
At DMPhysios, a well-recognized physiotherapy and rehabilitation center in Noida specializing in spine and sports-related conditions, special emphasis is placed on patient-centered rehabilitation for children and adults living with congenital dysplasia of hip.
The team of experienced physiotherapists designs personalized treatment plans that address muscle imbalances, improve hip stability, restore functional mobility, and help patients regain independence in daily life. Through evidence-based exercises, supportive therapy, and continuous monitoring, DMPhysios ensures that individuals affected by congenital dysplasia of hip can recover not just physically, but also regain confidence in movement and overall quality of life.
Symptoms
The presentation of congenital dysplasia of hip can vary depending on the severity of the condition and the age of diagnosis. Common symptoms include:
- In infants and young children:
- Asymmetry in leg length
- Limited hip abduction (difficulty spreading the legs apart)
- Uneven skin folds in the thighs or buttocks
- Clicking or popping sounds during hip movement
- Delayed walking milestones
- In older children and adults:
- Limping or waddling gait
- Hip pain, especially with movement or prolonged standing
- Early onset of hip arthritis
- Restricted range of motion
- Muscle weakness around the hip and pelvis
Because congenital dysplasia of hip can be subtle in the early stages, routine screening by pediatricians and orthopedic specialists plays a vital role in timely detection.
Types of Congenital Dysplasia of Hip
Congenital dysplasia of hip can be classified into different categories based on severity and structural changes:
- Hip Instability – The hip joint is loose, but the femoral head remains within the socket.
- Hip Subluxation – The femoral head is partially displaced from the socket but not completely out.
- Hip Dislocation – The femoral head is completely outside the acetabulum.
- Acetabular Dysplasia – The hip socket is shallow, leading to instability without dislocation.
Recognizing the type of congenital dysplasia of hip is important for choosing the appropriate treatment and physiotherapy strategies.
Causes
The exact cause of congenital dysplasia of hip is multifactorial, involving both genetic and environmental factors. Some of the primary causes include:
- Genetic predisposition: A family history of hip dysplasia increases the risk.
- Intrauterine position: Breech presentation and restricted space in the womb may affect hip joint development.
- Hormonal influences: Maternal hormones like relaxin can increase ligament laxity in the fetus.
- Abnormal fetal growth: Larger babies may exert more pressure on the hip joint during development.
Risk Factors
Several risk factors increase the likelihood of congenital dysplasia of hip, including:
- Female sex (higher prevalence in girls)
- First-born babies (less uterine space for movement)
- Breech birth presentation
- Family history of hip dysplasia
- Swaddling practices that tightly wrap the legs in extension and adduction
- Associated musculoskeletal conditions (e.g., clubfoot, torticollis)
Understanding these risk factors helps in preventive care and early screening strategies.
Treatment
The treatment of congenital dysplasia of hip depends on the age of diagnosis and severity of the condition.
- In Infants (0–6 months):
A Pavlik harness is commonly used, keeping the hips in a flexed and abducted position to encourage proper joint development. - In Older Infants (6–18 months):
If a harness is ineffective, closed reduction under anesthesia may be performed, followed by immobilization with a hip spica cast. - In Toddlers and Older Children:
Open reduction surgery may be necessary to realign the hip joint and correct deformities. - In Adolescents and Adults:
Surgical options like osteotomies or even total hip replacement may be considered in severe cases.
Early diagnosis greatly improves outcomes, reducing the need for invasive surgical interventions.
Physiotherapy Treatment (Detailed)
Physiotherapy plays a central role in the management and long-term recovery of patients with congenital dysplasia of hip. At DMPhysios, patient-centered rehabilitation programs are designed according to age, type of dysplasia, and stage of treatment.
1. For Infants and Young Children:
- Parental education: Guidance on safe handling, carrying, and positioning of the child.
- Support with Pavlik harness: Teaching families exercises that maintain hip flexibility without compromising the harness.
- Gentle range of motion (ROM) exercises: Encouraging abduction and flexion of the hips.
2. Post-Casting Rehabilitation:
- Gradual mobility exercises after removal of spica casts.
- Passive stretching to restore joint flexibility.
- Muscle strengthening to rebuild hip and pelvic stability.
3. For Older Children and Adolescents:
- Strengthening Exercises: Focus on hip abductors, extensors, and core muscles to stabilize the pelvis.
- Gait Training: Corrective walking drills, balance training, and use of assistive devices if necessary.
- Functional Training: Squats, bridging, and step-up activities tailored to restore normal movement patterns.
4. For Adults with Hip Dysplasia or Post-Surgery:
- Pain Management: Modalities such as ultrasound, TENS, and cryotherapy for pain relief.
- Progressive Strength Training: Gluteal strengthening, resistance band workouts, and hip stability drills.
- Flexibility Training: Controlled stretching to reduce stiffness and improve range of motion.
- Core Stabilization: Pilates and functional core exercises to improve pelvic alignment.
- Sports Rehabilitation: Customized programs for athletes recovering from hip dysplasia-related surgeries.
At DMPhysios, rehabilitation is not just about exercises—it’s about building confidence, preventing recurrence, and enhancing long-term mobility.
Prevention
While congenital dysplasia of hip cannot always be prevented, certain measures reduce risks and complications:
- Routine screening in newborns and infants for early detection.
- Avoiding tight swaddling techniques that force the hips into extension and adduction.
- Encouraging safe baby carrying methods that support hip abduction.
- Regular follow-ups with pediatricians and orthopedic specialists in high-risk babies.
- Early referral to physiotherapy clinics like DMPhysios for guided rehabilitation.
Conclusion
Congenital dysplasia of hip is a condition that, if diagnosed early and treated properly, allows children and adults to lead active, pain-free lives. The key lies in awareness, early screening, appropriate interventions, and structured rehabilitation.
At DMPhysios, a trusted Noida-based clinic specializing in spine and sports conditions, patient-centered rehabilitation is at the core of care. Whether it’s guiding parents of newborns, helping adolescents regain mobility, or supporting adults after corrective surgery, the expert physiotherapists at DMPhysios provide individualized care plans for congenital dysplasia of hip recovery.If you or your loved one is dealing with congenital dysplasia of hip, don’t wait for symptoms to worsen. Early rehabilitation ensures better outcomes. Book a consultation with DMPhysios today and take the first step toward a stronger, healthier future.